 Stroke is one of the most disabling illnesses a human being can suffer from. It impacts on the most frequently used parts of the body; the brain, limbs; movements, speech and emotions. The good news is that it can be avoided to a large extent, with healthy lifestyles. For those who have already had a stroke, it is also eminently treatable with good outcomes if detected early and the patient is brought to hospital as quickly as possible. Secretary, National Stroke Association of Sri Lanka and Consultant Neurologist, National Hospital, Dr Gamini Pathirana discusses the impacts of stroke and why early detection and treatment is so important to minimize complications, in this interview with the Sunday Observer.
Stroke is one of the most disabling illnesses a human being can suffer from. It impacts on the most frequently used parts of the body; the brain, limbs; movements, speech and emotions. The good news is that it can be avoided to a large extent, with healthy lifestyles. For those who have already had a stroke, it is also eminently treatable with good outcomes if detected early and the patient is brought to hospital as quickly as possible. Secretary, National Stroke Association of Sri Lanka and Consultant Neurologist, National Hospital, Dr Gamini Pathirana discusses the impacts of stroke and why early detection and treatment is so important to minimize complications, in this interview with the Sunday Observer.
Excerpts…
Q. This year’s theme for World Stroke Day, ‘Face the facts. Stroke is treatable’ sent out a very positive message. Your comments?
A. A research published in 1995 called ‘NINDS trial’ proved beyond doubt that strokes happening from the block of an artery by a blood clot could be dissolved with beneficial effects if the patient arrives before 4 ½ hours from onset. It has also been found that Stroke care in an ‘acute stroke unit’ too reduces disability. In other words, early treatment inclusive of dissolution of the clot, early aspirin therapy and acute stroke unit care reduces disability and mortality.
Q. Not many still understand what stroke is. What is stroke? How is it caused?
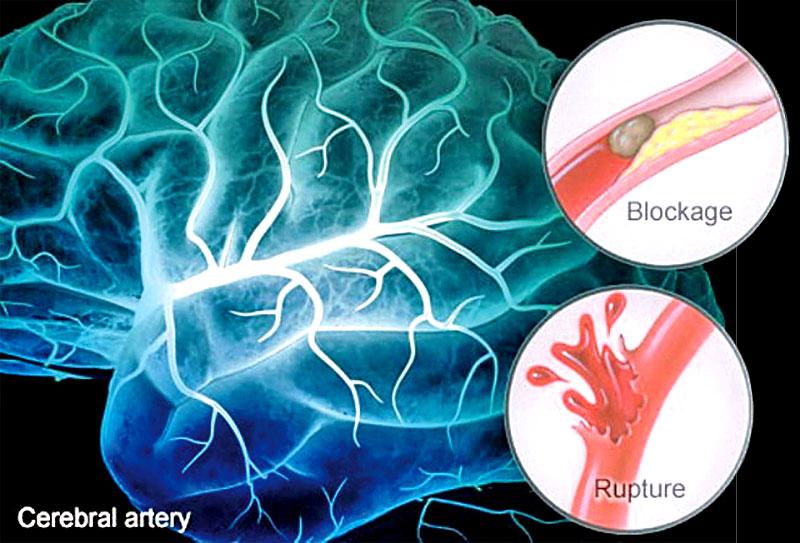
A. It is mostly caused by a dislodged clot migrating distally and blocking one of the arteries supplying brain. This results in the death of the area of brain supplied by that artery.
The dead area loses its function which results in paralysis of the opposite side of the body, loss of vision, difficulty in swallowing, difficulty in speaking etc. In others, stroke occurs from rupture of a vessel resulting in a bleeding into the brain, called ‘intracerebral haemorrhage.’ Regarding its causes, uncontrolled high blood pressure predisposes one to both types of stroke.
It is not acute rise, but the chronically elevated BP which causes this. During a stroke, we observe an acute rise in blood pressure which is called ‘reactive hypertension’. This is a natural mechanism to increase blood supply to the brain through the block.
This immediate elevation of blood pressure in a patient with ischemic stroke is not dropped by drugs up to 24 -48 hours unless there is a definite reason to do so. Hence, immediate detection is very important, because early detection reduces ‘time to hospital, which in turn reduces the impact of stroke on the patient.
Q. Who are those most at risk of getting a stroke age-wise and gender wise? Why?
A. The older you are, higher the chance of getting a stroke. Females are protected by hormones until menopause compared to male counterpart from any vascular event including stroke but after menopause both parties are equally vulnerable.
Q. Are genes a risk factor if one has a family history of strokes?
A. Strokes do occur in families. But mostly, they are related to the sharing of the risk factors I mentioned rather than genes. For example, we see same eating habits, same physical activity indices and exercise patterns within families. Also, diabetes and dyslipidemia can go in the family too. Directly genetically inherited causes for stroke are rare.

Q. Causes for strokes have been categorized as avoidable and non avoidable. What are they?
A. Non avoidable causes are aging, male sex etc. Avoidable causes are poorly controlled high blood pressure, diabetes mellitus, increased fat, lack of physical activity, mental stress, bad eating habits, obesity, smoking, and alcohol.
These are also called Modifiable risk factors. Stroke in patients with Atrial fibrillation (an abnormal heart rhythm) is also a risk factor.
It is a myth that ‘we can feel when the blood pressure rises’. ‘It is sufficient to take blood pressure pills when we feel our blood pressure rising’ is also wrong.
Blood pressure being the most important risk factor, can be raised to very high levels without causing symptoms and you will not feel this until it is measured.
Q. Can having a non communicable diseases like diabetes, heart problems, hypertension, aggravate effects of a stroke ?
A. Yes. The blood pressure and sugar level during an acute stroke certainly affect the outcome. This is why doctors monitor the blood pressure and the sugar closely after the stroke.
Q. Once a person gets a stroke, can he get it again?
A. If someone has had a stroke the chance of recurrence increases when compared to those who never had it. Those who have had a ‘cardiac event’ are also at higher risk of developing ‘cerebral events’ and vice versa. But, this increased risk can be brought down by risk factor modification. A second attack could be worse, so preventing recurrence is the best.
Q. Are there different types of strokes?
 A. Broadly there are two types. First, block of an artery called ‘cerebral infarct’ and second, rupture of an artery called ‘cerebral haemorrhage’. Differentiation of these two types done by an immediate CT scan of the brain, is the first step in management. There are differences in the management of the two groups.
A. Broadly there are two types. First, block of an artery called ‘cerebral infarct’ and second, rupture of an artery called ‘cerebral haemorrhage’. Differentiation of these two types done by an immediate CT scan of the brain, is the first step in management. There are differences in the management of the two groups.
For the first group, we give aspirin as early as possible and for the second group it is harmful to give aspirin.
For the first, ‘clot buster therapy’ is available, whereas for the second, it is harmful to give such an agent. ‘Dropping blood pressure immediately after stroke’ is not advisable in the first group, but it is done in the second group.
Q. What likely complications does a stroke victim have?
A. They are at risk of several complications. Due to poor swallowing, food and liquids are likely to go down the gullet causing pneumonia risk, body weight on pressure points causing pressure sores: The weight of a paralyzed arm on the shoulder causes shoulder pain: immobility of the leg leads to clot formation within calf vessels. These complications add to a negative outcome which can be minimized effectively in an organized stroke care unit.
Q. How soon should a victim be rushed to hospital for suspected stroke symptoms?
A. As soon as possible. Those who arrive before 4.5 hours if they have an ‘infarct’ are eligible for clot buster therapy.
Even if there is a delay beyond 4.5 hours, patients need to come to hospital as quickly as they can as we have other treatments to improve stroke outcomes for such patients. Coming late to hospital after days or months is not advisable.
Q. How is Stroke diagnosed?
A. Initially, by history and examination, followed by a CT scan of the brain. Patients brought to hospital have many services available to ensure good outcomes.
They include: urgent assessment including, swallowing, clot buster therapy, early aspirin therapy, blood pressure control, sugar control if diabetic, early physiotherapy, prevention of pneumonia, pressure sores and clot formation in calf, etc.
Q. Who treats them?
A. Treatment is done by a ‘stroke team’, usually, led by a neurologist or a physician interested in managing stroke. The stroke team meet regularly to discuss the patient’s progress and to take decisions in further care.
Q. The Stroke Unit at the National Hospital Colombo is reputed to be one of the best in South East Asia for its multi disciplinary approach to treating and rehabilitating patients. How do patients benefit from being treated at this Unit?
A. The Stroke unit at NHSL initiated by Dr.Udaya Ranawaka and currently headed by Dr. Padma Gunarathne is an example for developing similar units at other hospitals. By locating stroke patients to one area, and having a dedicated stroke team to look after them, it has been shown by repeated scientific research that the outcome can be improved
Q. What is the role of the National Stroke Association of Sri Lanka in which you are Secretary, in promoting stroke care for patients?
A. The National Stroke Association of Sri Lanka now headed by Dr MTM Riffsy, is a charity organization comprising most neurologists in the country and well-wishers. We don’t treat patients. Our goal is to improve stroke services and increase awareness about stroke among public and hospital staff about the services available in the country.
Q. Proper stroke care is still hampered by various factors in Sri Lanka. Your comments?
A. Since resources are limited, we try to optimally utilize the available facilities. Currently, the Health Ministry is funding a program to develop stroke units throughout the island with directions from National Stroke Association. This is a timely move and a very cost effective option.
Q. Once a person gets a stroke how long will he take to recover?
A. Recovery rate varies from patient to patient. It also depends on the type of stroke, severity, care received during the acute post stroke period, the patient’s will power and motivation, and support from family. The goal of rehabilitation is to allow a patient lead a normal and independent life. When we cannot improve function by improving patient, we look at using what are called orthotics or changing his environment to suit his disability.
Q. Is physical therapy part of that rehabilitation?
A. Physical therapy is a main part of rehabilitation. Exercises suitable for them are decided by a physiotherapist and the stroke team, and are tailor made for each patient.
Q. How are they fed? Do they require a special diet?
A. Feeding in the acute stage should happen after swallowing assessment because some patients lose their swallowing capacity after stroke with a risk of pneumonia, a common fatal complication after stroke. Stroke patients are either fed through oral route or through a Nasogastric tube or via a PEG tube (goes through tummy) Their diet should match the problems they have e.g. diet free of sugar for diabetics. Otherwise they would normally have a balanced diet.
Q. New advances in detecting and treating strokes early?
A. Intra venous thrombolysis, where a clot buster given through a vein is a relatively new option. This treatment is available only for some patients with infarcts.
All infarcts presenting within 4.5 hours should be screened and doctors going through a screening assessment select some of them for this therapy.
The decision to give clot buster is a medical decision by doctors so it won’t be given on patient demand. This treatment is now available in some major hospitals including the National Hospital.
‘Mechanical clot retrieval’ is another option which needs high expertise and equipment and is costly. This is not widely available in SL.
Q. Golden rules to follow if a stroke symptom is suspected?
A. If you suspect stroke, note the time at which it happened and bring him or her to the nearest hospital as quickly as possible. If you have arrived within hours you may request to be seen early. Don’t attempt to give food or liquid until swallowing screening is done.