With dengue cases and deaths reported islandwide mounting compared to the previous year (35,267) suspected cases up to August 5 this year, the Health Ministry and related units have launched several clean up campaigns noting that the current weather conditions of short spells of rain followed by sunshine are ideal for the root cause of dengue spread; namely, breeding sites . Added to this is the fact that at present the dengue virus circulating is DENV-2 and DENV-3, unlike in 2017 when the large outbreak was caused only by the DENV-2 virus, which Medical Officers believe is one reason why its spread is difficult to control. While schools, construction sites and places of religious worship will be some priority areas being targeted by the Beat Dengue campaigns, a health official says the most effective method to control its spread is to eliminate breeding sites created by ourselves.
 Chief Medical Officer of Health, Ratmalana, Dr Indika Ellawala explains how the disease is spread and shares some simple rules to follow to prevent its harmful impacts in this interview with the Sunday Observer.
Chief Medical Officer of Health, Ratmalana, Dr Indika Ellawala explains how the disease is spread and shares some simple rules to follow to prevent its harmful impacts in this interview with the Sunday Observer.
Excerpts…
Q. The current weather conditions in the country are ideal for mosquito breeding sites. This has prompted fears of an outbreak of dengue . Although most of us are now aware of dengue due to the awareness raising campaigns by the Health Ministry, many still don’t know how it is transmitted and what causes it . Can you explain this to our readers?
A. Dengue is an arboviral disease. There are four virus serotypes designated as DENV-1, DENV-2, DENV-3, and DENV-4. Transmission of the dengue virus depends on biotic and abiotic factors including the virus, the vector and the host. Dengue Fever (DF) and Dengue Hemorrhagic Fever (DHF) is transmitted by the female mosquito Aedes aegypti and Aedes albopictus. Aedes aegypti is the major vector of DF/DHF that cause epidemics. Aedes albopictus may cause epidemics when its density is high. Abiotic factors are temperature, humidity and rainfall.
The female mosquito gets infected when it bites a person who has the virus in his or her bloodstream. In addition, the eggs laid by an infected female mosquito leads to the hatching of mosquitoes that carry the virus. When these mosquitoes bite an uninfected person, they release the virus into the bloodstream. The first symptoms of the disease appear 5-7 days after an infected mosquito bite.
Depending on the temperature and humidity adult life span can be 2-4 weeks. The life cycle has four distinct stages; egg, larva, pupa and adult. The first three stages are aquatic and adult is terrestrial. The life cycle is usually 7-10 days depending on the environmental factors.
Q. What does this mosquito look like?
A. Adult Aedes mosquitoes are small to medium in size (4-7mm), dark in colour with white marking bands on the body.
Q. What are the types of dengue currently circulating in Sri Lanka? Is there a difference in the types circulating now compared to previous years?
A. In 2017, we had a large epidemic due to DENV-2. Nowadays we have dengue fever due to DENV-2 and DENV-3. That is the reason why it is difficult to control.
Q. Does the level of dengue fever vary? What are the health impacts at each stage? Explain in detail.
A. Dengue viral infection may be asymptomatic or may cause a spectrum of symptomatic clinical disease with the following possible outcomes:Un-differential fever Dengue Fever(DF)Dengue Haemorrhagic Fever (DHF)Expanded Dengue Syndrome
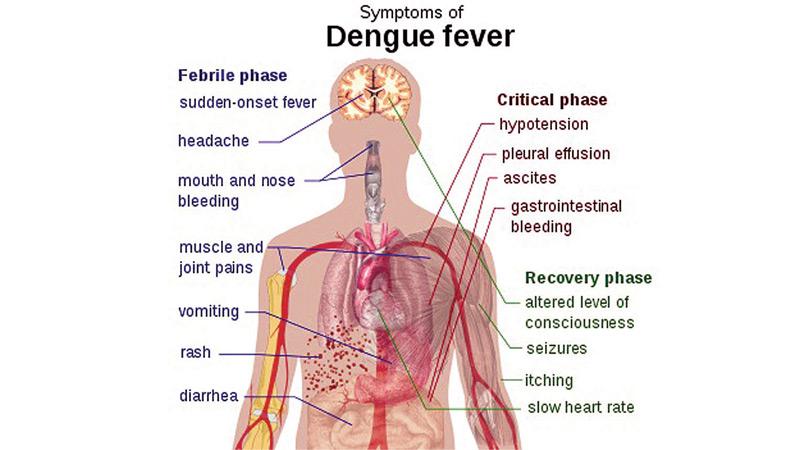
Among symptomatic dengue patients, DF and DHF are the most significant two clinical appearances encountered. During the initial days termed as febrile phase both groups are clinically similar. DF patients progress to convalescent phase where fever settles. DHF patients develop the critical phase due to altered vascular permeability leading to plasma leakage.
Q. How can you tell the difference between a common flu and dengue fever as both have similar symptoms at the start?
A. Dengue fever is generally an acute febrile illness with non-specific clinical signs and symptoms. Acute onset of high grade fever with body ache, diffuse blanching erythema of the skin, back pain, myalgia, arthralgia, headache, vomiting, loss of appetite, and diarrhoea. Some patients may have sore throat, and can be associated with upper or lower respiratory tract infections. Minor bleeding can manifest as petechial haemorrhage, mucosal bleeding and nasal bleeding. However bleeding can be heavy in some patients who are on Aspirin, steroids and NSAIDs.
In DHF in the first few days the patient will have signs and symptoms similar to DF. However in DHF the patient develops features of plasma leakage and bleeding. DHF patients have three stages:
Febrile phase
Critical phase
Convalescent phase
Critical phase occurs towards the late febrile phase, often after the end of the 2nd day of fever, usually around the 4th and 5th day with the fever settling. Some patients may enter the critical phase while having high fever. However, in pregnancy this may occur outside the usual duration earlier or later. Therefore, frequent Full Blood Count (FBC,) assessments, regular HCT and ultrasound scan abdomen and pelvis are important for early diagnosis.
Q. Warning signs?
A. Clinical deterioration with settling of fever, severe abdominal pain, excessive vomiting, cold clammy peripheries, no urine output for 4-6 hours and bleeding manifestations are warning signs of significant capillary plasma leakage.
Q. When should a patient be hospitalised?
A. Patients with a rapid drop of platelet count over a short period of time should be admitted.
Q. Treatment wise – what is the usual procedure when a patient comes with suspected dengue symptoms?
A. Patients with platelet count more than 130,000/Cumm can manage under the guidance of a qualified medical officer at home. They can take fluids, not only water but white rice kanji, soup, ORS, king coconut water. Red or brown colour foods and beverages are not recommended. Amount of fluid per hour is calculated according to body weight. Usually a person above 50kg needs 100ml of fluids per hour. Patient should measure urine output 4 hourly, and should be at least 1ml/kg/hour. If the urine output is lower patient should take more fluids to maintain the above urine output. To control the fever, only paracetamol is recommended. NSAID is not recommended under any circumstances. Physical rest is important, and patient should not be left alone at home.
Q. Who are most at risk of getting dengue? Pregnant mothers? Elderly?
A. High risk patients are pregnant mothers (better to admit on D1 fever), children less than 18 months, elderly patients, patients with severe diarrhoea and vomiting, patients with chronic renal failure, Ischemic heart disease and other serious medical conditions.
Q. What is the best approach to control the spread of dengue?
A. As no specific medicine or vaccine is available, we can control this disease only by vector control activities.
Q. Such as?
A. Dengue vector breeding sites are found within and outside household premises, at ground level and places such as roof gutters, overhead tanks and slabs. The Aedes aegypti prefers artificial containers to lay their eggs. A single female mosquito lays eggs in a number of containers in a single cycle. Aedes albopictus usually breeds in natural containers such as leaf axis and tree holes. It also breeds in artificial containers in urban areas. Regular checkup and destroying containers where water can collect is the best option for mosquito control.
Q. Obstacles preventing proper dengue control activities?
A. While managing patients is important, preventing the disease occurring in the first place is the most effective method to combat it. In most cases, the source of dengue is in the house of the patient itself. We make it a point to clean our premises when we hear that a visit from the Public Health Inspectors is due, since we fear legal action. This calls for a change in attitude and responsible behaviour on our part to keep our surroundings clean to protect ourselves, and not because of the fear of dengue inspections.
Q. What are the methods used to eliminate breeding sites?
A. Chemical control, especially, thermal fogging can be used when cases are reported. However, only infected mosquitoes can be destroyed by spraying. Continuous clean up campaigns removing all containers where water can be collected is the most important intervention. As the mosquito is a day biter we have to use mosquito repellants during daytime to protect from mosquito bites.
Q. Basic rules to follow if you suspect you have dengue?
A. Seek medical advice in case of a fever, especially in dengue endemic areas, and if you develop any symptoms associated with dengue fever. Refrain from using painkillers except paracetamol in case of fever.
Most importantly remember the ongoing battle against dengue can only be won by destroying all mosquito breeding grounds around you, as the most vulnerable point in the dengue cycle is the larvae stage, which is in the breeding grounds which we ourselves have created.